Cancer-Related Fatigue
Marion Debus
Last update: 04.02.2020
Cancer-related fatigue (CRF) is considered by 58% of all outpatient cancer patients to be their most relevant symptom in everyday life, and they also experience it as being not adequately treated.
Under adjuvant chemotherapy or radiation therapy, CRF is the most frequent symptom, affecting 70–92% of patients. In palliative care nearly every patient is affected (>70%, and almost 100% in cases of palliative chemotherapy). Among relapse-free patients, especially those with a lymphoma or a breast cancer diagnosis, 20–36% still have relevant CRF 1–8 years after the initial diagnosis, which leads to increased inability to work and early retirement among the often still-young patients (1, 2).
Patients experience cancer-related fatigue on three different levels:
- Reduced vitality (physical body and etheric body): The patient experiences a general lack of ability to do much, with limb heaviness and a persistent feeling of exhaustion and feeling shattered, resulting in difficulty in completing daily tasks. After exertion, a feeling of fatigue persists for hours afterwards, which can extend to the next day if more effort is made.
- Mental problems (soul body): Motivation and drive disorders, depressive tendencies, social withdrawal.
- Cognitive impairment (I-organization): Attention and (short-term) memory disorders, which are particularly prominent over the long term.
A circadian rhythm problem
Cancer-related fatigue is associated with sleep/wake cycle disturbances. It is called Cancer-Related Insomnia (CRI), the reverse side of CRF. Complaints of insomnia are dominated by problems of frequent nocturnal awakening and reduced deep sleep phases; to a lesser extent there are problems falling asleep or waking up too early, but also a pathologically increased need for sleep, and sleeping too long (hypersomnia). The normal morning feeling of regeneration and refreshment is largely absent, which results in the described daytime tiredness.
The healthy polarity of days filled with activity and deep, restful sleep at night is lost – the night is pervaded by waking phases, while the phases of being awake during the day cannot be sufficiently active due to exhaustion and tiredness.
How does it happen that we normally get tired during the day and wake up revitalized and refreshed in the morning? During the wakeful time of the day, the human I-organization and soul body have a depleting effect on the vital forces of the etheric body through conscious activity. In other words, some of the forces of the etheric body that are active in growth, regeneration and metabolism are transformed by the ‘I’ and the soul body in the course of the day into forces of consciousness and muscle power.
Note: Mental alertness and the ability to concentrate (ability to think) tends to be highest at around 10 o’clock in the morning, while the consciousness that occurs in physical activity (muscular strength) is highest at around 5 o’clock in the afternoon. In the course of the day, therefore, the ‘I’ and soul body move their activity downwards, from the head area to the limb area.
During the night the soul body and I-organization normally withdraw from their conscious activity, day-consciousness is thereby extinguished, and muscle movements stop. In the phase of fatigue preceding sleep, the vitality consumed during the day is perceived as tiredness, a feeling of heaviness, loss of interest, along with concentration and memory limitations.
The need for sleep expresses the “longing” of the ‘I’ and the soul body to reconnect with the wisely shaping and invigorating forces of the cosmos, which once formed the entire organism during its sleeping embryonic phase. From this creative formative activity—experienced when awake conceptual activity goes to rest at night--people receive the impulses from which the body’s organs can be formed, animated and regenerated according to their spiritual archetypes.
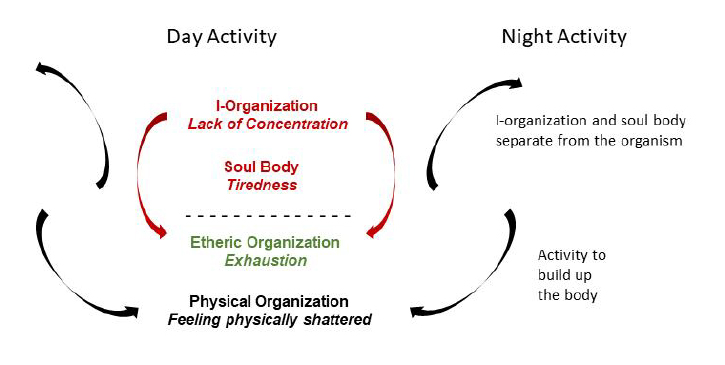
Fig. 1: Day and night activity of the I-organization and soul body (day activity = red, night activity = blue)
In cancer-related fatigue this interplay is profoundly disturbed: the I-organization and soul body do not connect during the day in a healthy way with physical body and etheric body, and they also cannot separate properly at night, whereby the body-regenerating formative activity which should be taking place during this time cannot become sufficiently effective. This leads on the one hand to the characteristic symptoms of fatigue and on the other hand it enables us to understand the well-known prognostic significance of CRF in cancer, because the nocturnal formative activity mediated by the soul body and I-organization is too weak. This finds physiological expression, for example, in the nocturnal secretion of melatonin, which on the one hand is associated with healthy sleep and on the other hand has immuno-stimulating and anti-tumoral effects (3).
General therapeutic approach
In terms of primary prevention, cancer-fatigue treatment should begin with the initial diagnosis (prehabilitation) and accompany the entire therapy phase (4). It should then focus on the phase following primary treatment or any adjuvant therapies – such as chemotherapy and radiation – that may be required. In palliative situations, it is part of complex symptomatic treatment.
Initial communication of the diagnosis
There is much evidence to suggest that conversations conducted in the context of communicating the initial diagnosis are of great importance regarding the further course of the disease and may determine the prognosis. There are initial indications from health services research that breast cancer patients receiving adjuvant chemotherapy who are given a detailed medical consultation and biography discussion as part of receiving their initial diagnosis have significantly fewer fatigue symptoms after six months (5). To be able to integrate the often-traumatic event of a cancer diagnosis into the entirety of one’s own biography seems to be essential.
Psycho-oncology and inner development
All psycho-oncological interventions and exercises should focus on the individual and current concerns of the patient. The primary aim is to support the patient on her way to herself, or to enable her to tread that path. Psycho-oncological treatment is therefore different at each point in time, whether during the diagnosis, the therapy phase, the integration of the disease into the patient’s own life or the palliative phase.
Important support is provided by exercises for mental and spiritual strengthening, as well as inner development, which the patient can perform himself with the help of instructions, for example:
- Exercises to strengthen thinking
- Abstention from all speculation
- Completion of incomplete perceptions
- Exercises for dealing with feelings
- Will exercises
- Positivity exercises
- Combined stress management exercises
- Inner calm exercises
- Review of the day
- Meditation (6).
Physical exercise
Through physical exercise, usually recommended as aerobic training for 30–45 min. 3 to 5 times a week, the I-organization and soul body are brought into the physical body and etheric body in a healthy way, which has a positive effect on fatigue and is currently considered to be the gold standard of fatigue treatment in conventional medicine (1, 2). Purely mechanical exercise on an exercise bike stands in contrast to movement in the great outdoors, which, in addition to physical locomotion, can also stimulate the soul in a healthy way through vivid sensory impressions – such as observing the changing vegetation throughout the year or observing the weather and light conditions – while at the same time having a calming and relaxing effect.
Mistletoe therapy
Mistletoe therapy – either as an adjunct to chemotherapy, anti-hormonal therapy, antibody therapy, radiation therapy, etc., or as the sole therapy – has shown positive effects on fatigue and sleep quality in numerous studies and is therefore used for prophylaxis in Anthroposophic Medicine and as the basis for cancer-fatigue treatment in all stages.
See also: www.misteltherapie.de
Rhythm
As shown above, rhythm disturbances, especially of the day-night rhythm, are the central problem of cancer fatigue. An interprofessional treatment concept should therefore particularly focus on this aspect. In a recent multicenter, randomized study with breast cancer patients in the adjuvant situation (7), such a multimodal concept – with eurythmy therapy, painting therapy, psychoeducation and sleep education – was studied in comparison to aerobic training. It showed a significant superiority of the multimodal program in essential parameters of fatigue compared to aerobic training. In the 10-week intervention program, the intervention group completed the following program once a week:
16.00 – 16.16 Welcome and Evaluation
16.15 – 17.00 Eurythmy Therapy
17.00 – 17.15 Break
17.15 – 18.30 Psychoeducation and Sleep Education
18.30 – 18.45 Break
18.45 – 19.30 Painting Therapy
19.30 – 19.45 Debriefing and Evaluation
The therapies were all aimed at taking up the topic of rhythm and making it tangible for the patients in their activity. In addition to conveying a general basic understanding of chronobiology, sleep education also included specific, independent applications of rhythm and consistency in the person’s individual everyday life.
Although the results still need to be confirmed in larger patient populations, this concept can already serve as a reliable basis for multi-professional rehabilitation programs for cancer-fatigue patients.