Principles and Application of Mistletoe Therapy in Oncology
Marion Debus
Last update: 07.10.2019
Introduction to Subcutaneous Application in Mistletoe Therapy
Subcutaneous application is the standard procedure which has been used the most widely to treat cancer patients with mistletoe. This form of mistletoe therapy has been approved by the German Federal Office for Drugs and Medical Devices (BfArM) and most clinical studies are based on it. In this article we will explain the most important practical aspects, so that you can safely introduce mistletoe therapy for your tumor patients on an outpatient basis, even with little previous experience.
There are many other ways of treating with mistletoe – intralesional, intracavitary, intravenous, high doses with fever induction – which are described in detail in the Vademecum of Anthroposophic Medicines. Treatment modalities described in the volume on Best Practices for Mistletoe Use in Cancer Care (1) , as well as off-label applications, considerably expand the possibilities for therapy. Those treatments cannot be discussed in detail in this introductory presentation.
The website www.mistel-therapie.de offers an overview of the therapeutic use and scientific evidence of mistletoe in various tumor types.
Medical indications
- all tumor stages (adjuvant and palliative situations),
- perioperative,
- during and after radiation therapy and/or chemotherapy/antibody therapy,
- cancer-related fatigue.
Injection site
Wherever possible, subcutaneous injections should be given close to the site of the tumor, e.g., in the skin of the abdomen to treat abdominal tumors.
Please note: the extent of the local reaction (see below) may be different at different injection sites.
Warning: Irradiated regions of the body should be avoided in all cases.
1–2 weeks before surgery, preoperative mistletoe injections should no longer be given in the future surgical area (e.g., abdominal skin), because of possible local reactions.
Initial Dosages with Preparations from Different Manufacturers
- abnobaVISCUM®
Available dosages: strengths 0.02 mg, 0.2 mg, 2 mg, 20 mg, as well as potency levels D6, D10, D20, D30.
Start with abnobaVISCUM® 0.2 mg (or 0.02 mg in case of a sensitive constitution) 3 x/week. 1 amp s.c.
Increase over time by maintaining 0.2 mg (0.02 mg) 1–2 x/week and adding 2 mg (0.2 mg) 1 x/week. Then increase respectively to 2 mg 1–2 x/week and 20 mg 1 x/week. - Helixor®
Available dosages: strengths 0.01 mg, 0.1 mg, 1 mg, 5 mg, 10 mg, 20 mg, 30 mg, 50 mg, 100 mg.
Start with Helixor® series 1 (1–10 mg), 1 amp s. c. 3 x/week, if well tolerated followed by series 2 (1–20 mg), if well tolerated followed by series 4 (20–50 mg). - Iscador®
Available dosages: strengths 0.0001 mg, 0.001 mg, 0.01 mg, 0.1 mg, 1 mg, 10 mg, 20 mg.
Start with Iscador® series 0 (0.01–1 mg), 1 amp. s. c. 3 x/week, if well tolerated followed by series I (0.1–10 mg), if well tolerated followed by series II (1–20 mg).
As an alternative: start with Iscador® series 0 every 2nd day for 2 weeks, then stop for 1 week. If well tolerated, follow with series I and II in the same way. - Iscucin®
Available dosages: strengths A, B, C, D, E, F, G, H.
Start with Iscucin® series I (strength A–D), 1 amp. s. c. 3 x/week, then series II (strength D–G) 3 x/week, until the desired reaction is achieved.
Note: After completing the two series, patients are often treated with potentized mistletoe (strength A–C) 1–2 x/week, in combination with a materially emphasized dose (strength E–H) 1 x/week.
What Are the Proven Parameters for Managing Mistletoe Therapy?
1. Local reaction
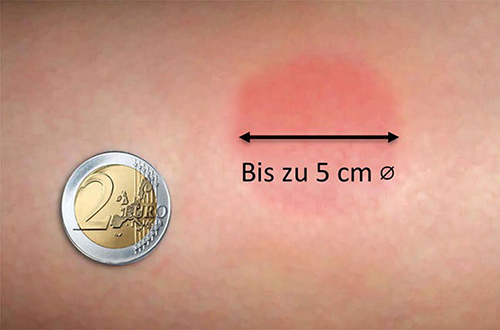
Fig. 1: Desirable local reaction after a mistletoe application . © Photo: Michael Siffrin
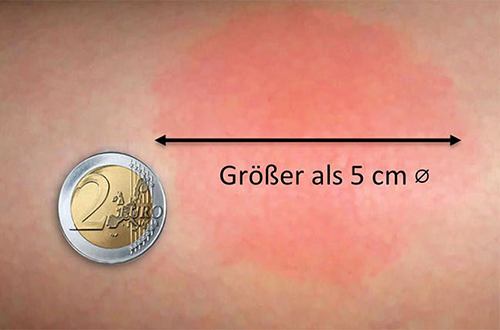
Fig. 2: Excessive local reaction after a mistletoe application. © Photo: Michael Siffrin
A good orientation point for the speed of dosage increase and the ultimate optimal dose is the local reaction occurring at the injection site, as an expression of immune stimulation: when this has reached a diameter of 3–5 cm, the current dose can be maintained for the time being. In most patients, the local reaction subsides during the course of treatment, and dosages can then be increased correspondingly. Approximately 5–10% of patients maintain a clear local reaction even when the dosage remains unchanged. According to available clinical observations, this persistence of the local reaction is often associated with a favorable prognosis (1, Chap. 7.1.3.1). Nevertheless, a reduction in the local reaction does not mean that the mistletoe is not having an effect.
The extent of the local reaction may vary in the same patient depending on the injection site. The local reaction can also increase again depending on the situation (e.g., after an infection). As a matter of principle, it is sensible to continually vary the injection site within a particular region of the body (e.g., the abdominal skin or upper thigh).
Individual patients react with different degrees of sensitivity to mistletoe, so that the same dosages can induce local reactions of very different intensity, depending on the patient: for one patient, a relatively low dose may be retained for months, while for another the dose can be increased to a maximum within only a few weeks. The decisive factor is not the dose, but the effect achieved.
2. The subjective experience of the patient
The most important criterion for managing mistletoe therapy is the clinically observable condition of the patient. This includes a range of parameters that can be helpful for evaluating treatment.
In general, the patient should have the sense that something is happening, that mistletoe is alleviating many of the symptoms of rigidity associated with cancer – such as loss of temperature rhythm or a depressive mood – and that things are starting to shift.
Effects on the immune system: improved warmth generation and regulation, reduced susceptibility to infections
Soon after the start of mistletoe therapy, patients often describe a clear sense of inner warmth or a diminution of their cold intolerance, which cancer patients often – but by no means always – have. Patients once more experience their body as having a warm interior, accompanied by a sense of well-being. This more subjective sensation can be followed by an objectively demonstrated rise in body temperature or a more rhythmically patterned temperature graph.
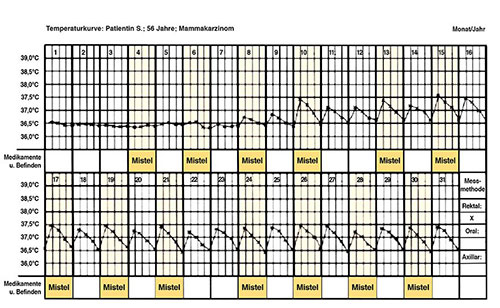
Fig. 3: Temperature graph (in months): patient S., 56 years old, breast cancer
However, the temperature graph is often an imprecise indicator and does not clearly correlate with the progression of the illness. It is only one criterion among several. Measurement of temperature before treatment, and then intermittently, can be helpful if the temperature is taken exactly (rectally) several times a day after an appropriate rest period – preferably before getting up and between 4 p.m. and 5 p.m. With some tumor diseases, such as malignant melanoma, a pronounced subnormal temperature (< 35°C or 95°F) with an inverse temperature rhythm is common. Using a temperature graph to monitor this can be particularly helpful in such cases. Often, it is enough to pay attention to the above described change in the patient’s subjective sensation of warmth.
The patient’s improved warmth regulation is also an expression of a stabilization of their immune system, with a significant reduction in susceptibility to infections. This is also an important reason why quite a few patients in the adjuvant situation continue mistletoe therapy even for years after.
Increased vitality, reduced fatigue
The patient’s vitality is often enhanced remarkably, connected with a sense of “rejuvenation” and a general increase in energy levels, as the expression of a strengthening of the etheric body. Chemotherapy is better tolerated and the associated or tumor-related fatigue can be reduced. Desirable weight gain can also occur. The insomnia which often occurs and is associated with fatigue often improves, and other possible disturbances in vegetative function can normalize. For example, appetite and libido can increase again (1, chap. 7.1.3.3).
Disease stabilization, tumor remission
The physical tumor itself may stabilize or even go into remission. This effect naturally only becomes apparent after a longer period. There have been numerous observations that such remissions are accompanied by improvements in the patient’s warmth organism, in cases where it had been clearly disturbed (1, chap. 7.1.3.3).
Effects of mistletoe therapy on the soul and spirit
The patient’s improved physical warmth generation and regulation will also appear on the level of soul. For instance, mistletoe therapy may have an antidepressant, brightening effect, leading to heightened reactivity of an emotional life that may have previously stagnated under the burden of illness. Anxieties diminish; patients develop confidence in their situation again. At the level of the ‘I’, this is usually accompanied by an increased personality presence and initiative in dealing with their disease and in reshaping their biography (1, Chap. 7.1.3.3).
3. Laboratory readings
When evaluating the efficacy of mistletoe therapy, the same criteria apply as for other cancer treatments (e.g., imaging procedures, tumor markers). The neutrophil to granulocyte/lymphocyte ratio provides a general indication that can be determined in any practice on the basis of a differential blood count, correlating with the progression of various tumor diseases. In general, the lower the proportion of lymphocytes, the worse the prognosis is. Occasionally, eosinophilia can be observed at the beginning of treatment, which is often associated with a good response. Other parameters, such as a high-cost immune status reading, are not reliable as predictors. When carried out they should always be evaluated in association with the patient’s overall situation.
4. Signs of overdose
If the injection is followed by lassitude, shivering, headache or diarrhea, which persist until the next day, or excessively strong inflammatory local reactions, this suggests an overdose. Pausing mistletoe therapy for a short time until these reactions subside, and subsequent dose reduction or change of host tree is usually sufficient to remedy the problem.
5. Infections
Mistletoe therapy should be paused during a severe infection, or one accompanied by fever. Occasionally, when mistletoe therapy is resumed, an increased local reaction may be observed, which is explained by the activation of the immune system during the infection.
Patient-Related Considerations Affecting Dosage of Subcutaneous Mistletoe Therapy
- A cautious dosage should apply in the following cases:
- sensitive, neurasthenic patients, who report being sensitive to many things,
- patients with autoimmune diseases (1, Section 12.3),
- patients with allergies. - Patients with truncal obesity who are eager to communicate and are easily excitable should be given slowly increasing dosages, since they often respond with pronounced local reactions.
- Mistletoe therapy in a higher concentration or with a rapidly increasing dosage is particularly suitable for patients who have a general tendency to sclerosis and mental numbness, who appear “frozen” and show inadequate regeneration during the night.
- Patients who react unfavorably to a deciduous mistletoe are recommended to switch to a coniferous mistletoe.
Tumor-Related Parameters to Be Considered when Setting the Dose for Subcutaneous Mistletoe Therapy
- For patients in an adjuvant situation with a low-risk profile , the dose can be low to start with, and can be slowly increased depending on their individual reaction.
- For patients with metastases but otherwise good general condition , it is advisable to rapidly raise the dose, and when appropriate also to give fever-inducing high-dose mistletoe therapy (1, Chap. 7.1.7.)
- Cautious dosage is indicated for patients with a brain tumor or brain metastases in critical localization with perifocal edema. After resection or radiation, once the perifocal edema has subsided, however, normal doses can certainly be given.
- Preoperative treatment prior to tumor resection: it is desirable to start mistletoe therapy before the operation; most commonly using a standard schema.
- Late-stage palliative and weakened patients with advanced tumor disease should be given a warming, enveloping, non-confrontational mistletoe therapy. Suitable in this context are conifer mistletoes produced by different manufacturers, in low-dose or potentized form, (e.g., Helixor® A, Iscador® P, Iscucin® Abietis or Pini, abnobaVISCUM® Pini s.c.) or as an infusion.
The aim of therapy is to assuage the symptoms and elicit tranquility. The more advanced the disease, the weaker the concentration or the higher the potency should be.
The mistletoe should be administered once daily or every second day, depending on the patient’s quality of, and will for, life.
Pauses in Treatment and Length of Therapy
The length of mistletoe therapy, and the inclusion of treatment pauses, is managed individually. It is governed on the one hand by tumor-related criteria such as tumor type and stage, and the associated risk of relapse or progression, and on the other by the patient’s subjective state, their own self-assessment and life situation. The following general parameters result from this:
Adjuvant Situation
Low risk of recurrence: When there is a low risk of recurrence patients are generally treated with mistletoe for a period of 5 years. After 2–3 years of treatment, pauses can be introduced, which are gradually extended. For instance, 2 months of treatment, then 1 month pause; then 1 month of treatment and 2 months pause. In many cases, it has proven helpful to undertake a course of mistletoe lasting 1–2 months each spring and autumn.
However, the condition of the patient remains an important factor when deciding when to terminate or continue treatment. There are patients who, after a certain period of mistletoe treatment, feel that they are now healthy and that there is nothing more that mistletoe can do for them. Sometimes they even develop a kind of aversion to the mistletoe injections. In such cases, mistletoe therapy can be stopped even before the 5 years are up, as long as the physician sees no other reason to urge the patient to continue with it.
Other patients find that their condition worsens even in brief treatment pauses and they notice an increase in the sense of coldness, in susceptibility to infections, and/or states of fatigue. Such patients will usually themselves insist on continuing mistletoe treatment beyond the 5-year period, at a level individually determined, for many years.
High risk of recurrence: Certain tumors, such as breast cancers and melanomas, are generally associated with the risk of late recurrence after curative surgery, even after 10–15 years. Other tumor entities, e.g., carcinomas of the oral cavity, can likewise recur after many years. In addition, there are inherited forms of breast cancer and other tumor types associated with a particularly high risk of relapse or development of further tumor diseases (e.g., ovarian carcinoma in the case of BRCA-positive breast cancer). It is also known that intensive chemotherapy, for instance to treat lymphoma and leukemia, involve an increased risk of secondary malignancies in later life.
In all these cases, there is much to be said for continuing mistletoe therapy for many years, or even lifelong, always corresponding to the state of the patient, and with individually determined but not over-long pauses in treatment.
Palliative situation
In the case of metastasis or locally inoperable cancer, pauses or cessation of mistletoe therapy should be considered with great caution, especially if the patient suffers severe life events or if their state rapidly worsens during a treatment pause (see above).
In general, treatment should continue uninterrupted in the palliative situation, with regular adjustments of the therapy to the progression of the illness.
In the end-of-life phase, too, it can be very helpful to give mistletoe frequently until the end, in weaker concentrations or in potentized form. This aids pain reduction and enhancement of quality of life.
Important Parameters for Host Tree Selection
Mistletoe therapy is based on white-berried mistletoe (Viscum album), which is divided into three subspecies (2):
- Viscum album subsp. album grows exclusively on deciduous trees.
- Viscum album subsp. abietis grows only on species of fir.
- Viscum album subsp. austriacum prefers pine trees and can sometimes be found on spruce or larch.
Conifers (fir and pine), with their markedly shaped needles and cones, which maintain a very constant appearance through all the seasons, show a relationship to the likewise very structured, “static” nerve pole in human beings. Deciduous trees, in contrast, are characterized by pronounced seasonal changes, particularly visible in their leaves, which indicates a correlation with glandular metabolic and reproductive organs in the human body.
Against this background, as well as supported by broad clinical experience, coniferous mistletoe is generally selected to treat malignant tumors in the upper human being – especially brain tumors – and deciduous mistletoe is selected for tumors of the metabolic organs.
Interestingly, these differences can also be seen in the material qualities of the mistletoe plants growing on the corresponding trees: the three subspecies of V. album differ fundamentally in the composition of their different viscotoxin isoforms, and in addition, deciduous mistletoes are generally more lectin-rich than coniferous mistletoes. They can therefore generally trigger stronger inflammatory reactions than coniferous mistletoes, which is important for clinical use.
Conversely, when our intention is to mobilize the patient’s formative forces, we can (among other things) use coniferous mistletoes, which also improve a patient’s general condition when their vitality is very low.

Fig. 4: Coniferous mistletoe (fir tree)

Fig. 5: Deciduous mistletoe
Deciduous or Coniferous Mistletoe?
A first key decision is whether a deciduous or a coniferous mistletoe should be used.
As regards prescribing practice, it should be noted that pine and apple tree mistletoe preparations can be obtained from all four mistletoe manufacturers, oak and fir mistletoe preparations are each available from three of the four manufacturers, and the range of other deciduous tree mistletoes is broad, varying greatly from manufacturer to manufacturer. The following table provides an overview:
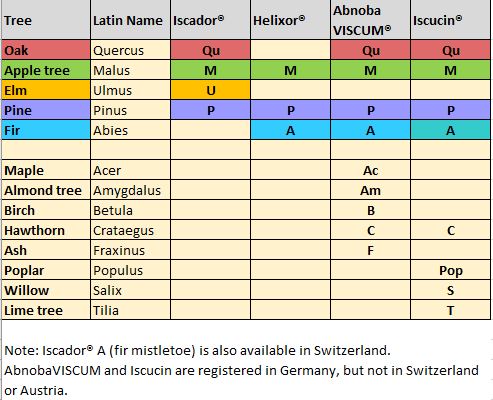
Fig. 6: Available host trees of the various mistletoe preparation manufacturers in Germany
Note: In Switzerland, fir mistletoe is also available from Iscador® (Iscador® A). AbnobaVISCUM and Iscucin are only approved in Germany, not in Switzerland or Austria.
The coniferous mistletoes: pine, fir
Mistletoe preparations made from coniferous mistletoes often have a good effect toward improving general well-being, and this is particularly apparent if used alongside chemotherapy or radiation therapy. It is not uncommon for mistletoe to help patients better tolerate these therapies and thereby even render them possible in the first place, through stabilizing bone marrow function and thus the leukocyte count, so that fewer infections occur and general health improves.
It is noteworthy that coniferous mistletoes, while displaying only low apoptosis-inducing effects in the experimental setting, nevertheless have a stabilizing effect on leukocytes during treatment with cytostatics (3) without impairing the antitumoral efficacy of conventional therapy (4).
The following general principles apply to treatment with subcutaneous mistletoe therapy:
Coniferous mistletoes are often favored
- when conventional cytoreductive chemotherapy or radiation therapy is currently being given and is at risk of undermining patient vitality,
- when vitality is considerably reduced, whether due to the constitution of underweight-asthenic, nerve-accentuated patients (neurasthenic constitution), or
- in a preterminal situation, or
- when the local situation prohibits a stronger inflammatory reaction with temporary swelling (e.g., gliomas)
- when deciduous mistletoes induce an excessive reaction.
The deciduous mistletoes: apple, oak, ash, etc.
Correspondingly, preparations made from deciduous mistletoes and given in higher concentrations (e.g., intratumorally administered) have a locally tumor-necrotizing and apoptosis-inducing action, and thus often induce a metabolically accentuated "digestion process". They trigger stronger inflammatory reactions than the gentler-acting coniferous mistletoes. Deciduous mistletoes are used first and foremost to exert a direct cytotoxic action in a localized tumor context. If a strong inflammatory reaction is undesirable or dangerous, perhaps because a peritumoral edema might cause articular constriction symptoms in a brain tumor, or stimulate increased pain from sensitive structures close to the tumor, medicines made of coniferous mistletoes are often more helpful. Deciduous mistletoes can also be overwhelming in cases where a patient’s general condition is severely impacted. They may tend to increase weakness, so that a coniferous mistletoe is more likely to be indicated.
Deciduous mistletoes are often favored
- when the patient’s vitality is good and we want to have an optimal effect on the tumor,
- when treating organ-related tumors in the gastrointestinal tract, lungs and reproductive organs,
- for intratumoral or peritumoral mistletoe therapy,
- when a pronounced febrile reaction is sought,
- when the local situation allows temporary swelling and inflammation,
- for intracavitary applications (mistletoe pleurodesis or pericardium, as well as urinary bladder instillation in superficial bladder tumors) under these circumstances (1, chap. 7.3–7.10).
When using deciduous mistletoes, it is especially important to adjust the dosage according to the patient’s levels of strength and energy, enabling the person to draw once more on their own vital resources. While intensive vitalization and immunological efficacy are possible, it must be noted that over-dosage taxes patients and can therefor weaken them. In such cases, it makes sense to switch to a coniferous mistletoe.
Alternation between Deciduous and Coniferous Mistletoes
In the last 20 years, strikingly good outcomes have been achieved with a rhythmic alternation between deciduous and coniferous mistletoe in cases where the patient’s general condition was impaired but not so severely that it prevented use of deciduous mistletoe, this alternation being used with the aim of controlling the tumor situation in the long term or even to cure the disease (5).
Differential Indications for Mistletoes from Different Host Trees
You can find a detailed description of the differential indications for various deciduous and coniferous mistletoes in the Vademecum of Anthroposophic Medicines, Best Practices for Mistletoe Use in Cancer Care (1, Chapter 5).
Bibliography
- Vademecum Anthroposophische Arzneimittel, vol. 2. 4th ed. Munich: Gesellschaft Anthroposophischer Ärzte in Deutschland; 2017. English translation: Vademecum of Anthroposophic Medicines. Best Practices for Mistletoe Use in Cancer Care. Munich: Verlag der Gesellschaft Anthroposophischer Ärzte in Deutschland; 2019.
- Zuber D. Biological Flora of Central Europe: Viscum album L. Flora 2004; 199: 181–203.
- Büssing A, Azhari T, Ostendorp H, Lehnert A, Schweizer K. Viscum album L extracts reduce sister chromatid exchanges in cultured peripheral blood mononuclear cells. European Journal of Cancer 1994; 30(12): 1836–1841.[Crossref]
- That mistletoe preparations do not reduce the efficacy of chemotherapeutics (doxorubicin, gemcitabine, docetaxel, mitoxantrone and cisplatin), regardless of the host tree, but have an additive effect in higher concentrations, was shown in vitro in mammary, pancreatic, prostate and bronchial carcinoma cell lines: Weissenstein U, Kunz M, Urech K, Baumgartner S. Interaction of standardized mistletoe (Viscum album) extracts with chemotherapeutic drugs regarding cytostatic and cytotoxic effects in vitro. BMC Complementary and Alternative Medicine 2014; 14(6): 1–9.[Crossref]
- Sommer M, Soldner G. Die Mistel und ihre Wirtsbäume. Differenzierungen zur Optimierung der Therapie. Der Merkurstab 2000; 53(1): 29–43.